


How Off-Label Use of Medicines Drives Health-Care Use and Disability
Peer-reviewed research finds that pharmaceutical innovation provides direct and indirect benefits for health-care use and disability.
KEY TAKEAWAYS
Key Takeaways
Contents
The Effect of Off-Label Use on Health-care Use and Disability 3
Off-Label Use, Vintage, and Implications for Pharmaceutical Detailing. 4
Introduction
There is controversy about whether pharmaceutical detailing leads physicians to prescribe medicines outside the label approved by the Food and Drug Administration. Off-label use is a significant public health burden, but there is no clear understanding of what is at stake when patients use drugs off-label. This briefing summarizes study results relying on data from the U.S. non-institutionalized population to examine the effects on health-care use and disability of using drugs off-label. Leveraging condition- and individual-specific effects that determine off-label use, it finds that replacing off-label use of drugs by on-label uses would reduce per capita medical expenditure and work loss cost by $515—about 13 percent. Newer (on-patent) drugs, which account for the vast majority of detailing efforts, are much less likely to be used off-label. Detailing activity as such may lead physicians to more targeted on-label use of drugs. Physician education policies could emphasize reducing off-label use of older drugs through synthesis of evidence of off-label uses independent from financial interests.
Off-label uses of drugs, which occurs when a patient uses an active ingredient outside the label that it has been approved for by the U.S. Food and Drug Administration (FDA), is a significant public health burden. Depending on disease area and study setting, the proportion of drugs used off-label in ambulatory care ranges between 21 and 44 percent.[1] Pediatric conditions, cancer care and rare diseases often have higher exposure to off-label use. To some patients, off-label use may be a last resort, especially when there are few approved treatment options. The problem with off-label use is that studies suggest that the vast majority of off-label uses lack scientific support: 61‒84 percent in ambulatory care, and 48 percent of choices in intensive care unit settings.[2] Off-label use is therefore unlikely to be effective, and may even harm the patient.
Given that off-label use may waste resources and harms patients, it is important to determine what causes off-label use and what the consequences for society are. A controversy arises around the role of pharmaceutical detailing and the promotion of off-label uses that are not supported by (strong) scientific evidence. On regulatory grounds, promotion of off-label uses is illegal. Nevertheless, some pharmaceutical manufacturers faced substantial regulatory settlements when allegations of off-label promotional activities were made.[3]
Could detailing activities lead to increased inappropriate use of drugs outside their designated labels? Answering this question is important from a policy perspective. If detailing of new drugs leads physicians to use drugs outside their designated label more often, despite the fact that promoting off-label uses is illegal, then the appropriateness of detailing physicians is put into question. Alternatively, measures such as anti-detailing or physician education could be modified to educate physicians about the areas where common off-label use are likely to cause no harm, but potentially cause significant waste through health-care use and disability resulting from inappropriate use of drugs. Such policies, for example within the scope of the Centers for Medicare and Medicaid Services, would require independent review boards to develop unbiased and comprehensive evidence reviews independent from financial interests.[4]
The evidence about the effects of detailing on off-label uses of drugs is controversial and concentrates on the use of antidepressants. In an evaluation of anti-detailing policies of academic medical centers, Larkin et al. (2014) demonstrated that the presence of such policies reduced off-label use of antispychotic drugs in children and adolescents by 11 percent compared to centers that did not have such a policy between 2006 and 2009.[5] This finding suggests that pharmaceutical sales representatives potentially promote drugs that are not approved for pediatric use. However, the study further shows that responses to on-label uses of drugs are double the identified effect of off-label uses (34 percent decrease). Off-label uses of drugs that were not promoted in pharmaceutical detailing activities increased by 35 percent as well. Besides, the study did not examine whether the academic medical centers that implemented an anti-detailing policy were having higher off-label uses to begin with, a source of biased effect estimate the study did not resolve on methodological grounds. Another study by Shapiro (2018) evaluated the role of two informational shocks of the side-effect profiles of drugs frequently used off-label. AstraZeneca was sued for unlawfully promoting off-label use of a drug named Seroquel and paid a fine of $520 million.[6] Although the study found that new information about side effects was primarily transmitted through promotional activity, the study also found that detailing did not substantially increase off-label uses. If anything, the distribution tilted from off-label towards on-label use.
Off-label uses of drugs, which occurs when a patient uses an active ingredient outside the label that it has been approved for by the FDA, is a significant public health burden.
In a recent study, we explored the effect of using a drug off-label on health-care use and disability.[7] We examined market size and innovation status measured by FDA approval year as attributes that lead to more or less off-label use at the condition level. In contrast to previous investigations of economic- and health-related consequences of off-label use that have emphasized cancer care and depression, our study covers a wide range of 247 conditions. We carefully account for the fact that some individuals may use off-label treatments more often than others and that some conditions lead to more intense use of health care and disability. Additionally, we dealt with an important endogeneity issue by demonstrating that individuals with higher disease severity and multiple conditions do not experience higher off-label use once we account for unobserved individual effects.
The data we relied on include combinations of prescription drug labels and indicated conditions for over 200,000 individuals in the U.S. non-institutionalized population between 1996 and 2015, linked to comprehensive data from a pharmaceutical reference database. The data that match approved indications to active pharmaceutical ingredients that we use are unique as these are independent from medical compendia. We observe about 13,000 combinations by active ingredient and condition approved in France for prescription use from an independent source, edited by the French Centre National Hospitalier d’information sur le Médicament.[8] We linked those data to active ingredient-condition pairs reported by patients in the U.S. Medical Expenditure Panel Survey. We measured off-label use as the fraction of drugs prescribed for a condition by individual according to condition-active ingredient pairs not recorded as on-label in our pharmaceutical reference data.
The Effect of Off-Label Use on Health-care Use and Disability
We found that off-label use generally increases medical expenditures and work-loss costs. Our empirical estimates of two-way fixed effects regressions and counterfactual analyses suggested that using only on-label drugs compared to the average 2015 off-label drug use would lead to savings of $515 per individual in terms of health-care use and work-loss cost. This value reflects 12.9 percent of all medical expenditure covered in our data. Estimates are robust across a number of specifications, for example when we exclude FDA approval year or include time-fixed effects.
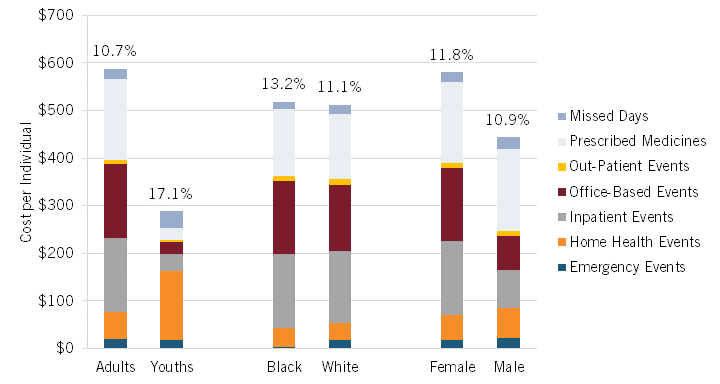
The dollar value of eliminating off-label use was based on seven outcomes of health-care use and disability by person and condition. Estimates are larger in children and adolescents compared to adults, in females compared to males, but not in blacks compared to whites. (Figure 1.) The difference in the cost of off-label compared to on-label treatments, $680 on average, does not outweigh the increased spending from off-label use. Off-label treatments as such are on average more expensive. The projected savings from reducing off-label use can be used as reference value for policy design to target reductions in off-label use.
Figure 1: Health-care use and disability attributed to off-label use, by population groups, 2015
Off-Label Use, Vintage, and Implications for Pharmaceutical Detailing
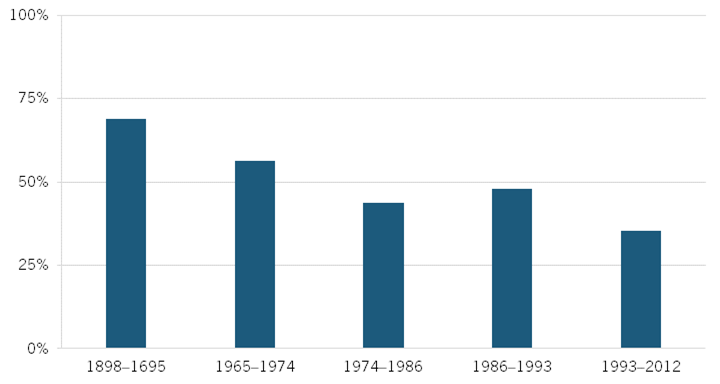
In the context of pharmaceutical detailing, our analysis demonstrates that off-label use is inversely related to year of regulatory approval, an indicator of a drug’s vintage. Figure 2 shows associations of off-label use across the spectrum of FDA approval years in five groups. The fraction of drugs used off-label that were approved before 1966 is about twice as great as that of drugs approved between 1993 and 2012: 68.5 percent compared to 35.4 percent. Pharmaceutical innovation may therefore have both direct effects on health-care use and disability and indirect effects via the propensity to use drugs off-label. An explanation for these stark differences lies in that pharmaceutical detailing is most intense for the latest approved drugs. Duflos and Lichtenberg (2012) found that marketing expenditure declines by about 50–60 percent in the years immediately following generic entry.[9]
Figure 2: Association of off-label use and FDA approval year
Conclusion
Off-label use of drugs not only causes adverse drug events, but also significant amounts of medical expenditure and work-loss cost to society. Although we cannot measure the effect of detailing on off-label use directly, considering approval status of a drug suggests that pharmaceutical detailing for which most spending by pharmaceutical manufacturers is made may not be the source of the substantial proportion off-label uses we and others have identified. Instead, if anything, pharmaceutical detailing may reinforce the evidence base according to regulatory information of the latest available treatments. Appropriate use of older drugs may be the more important target of anti-detailing or physician education policies. Such policies would require comprehensive evidence review of off-label uses of older drugs to guide prescribers towards the best available evidence and treatments. Whether such efforts are worth the savings potential we identified from eliminating off-label use is a question of policy implementation.
Estimates from our study and from previous studies also indicate that, in addition to reducing off-label use, use of newer drugs generally reduces expenditure on other types of medical care: inpatient, outpatient, emergency room, office-based visits, and home health care. Hence the net cost of using a new drug is significantly less than the price of the drug; it may even be negative once these “cost offsets” are taken into account. The introduction of a new drug also tends to put downward pressure on the prices of older drugs in the same therapeutic class.[10] Payors and policymakers should be aware of these beneficial “side effects” of new drugs when they evaluate the cost-effectiveness of those drugs to make coverage decisions, and when they design and implement innovation and intellectual property policies.
About the Authors
Katharina E. Blankart is an assistant professor in empirical health economics at the faculty of Business Administration and Economics of University of Duisburg-Essen; a full member of the health economics research center CINCH; and head of the junior research group “Empirical Analysis of Health Care Markets” ( EACH).
Frank R. Lichtenberg is Cain Brothers & Company Professor of Healthcare Management in the faculty of Business Economics at the Columbia University Graduate School of Business; a research associate of the National Bureau of Economic Research; and a member of the CESifo Research Network.
About ITIF
The Information Technology and Innovation Foundation (ITIF) is an independent, nonprofit, nonpartisan research and educational institute focusing on the intersection of technological innovation and public policy. Recognized by its peers in the think tank community as the global center of excellence for science and technology policy, ITIF’s mission is to formulate and promote policy solutions that accelerate innovation and boost productivity to spur growth, opportunity, and progress. For more information, visit us at itif.org.
Endnotes
[1]. Katharina E. Blankart and Frank R. Lichtenberg, “The Effects of Off-Label Drug Use on Disability and Medical Expenditure,” National Bureau of Economic Research, Working Paper Series, 2022, https://doi.org/10.3386/w30440; W. David Bradford, John L. Turner, and Jonathan W. Williams, “Off-Label Use Of Pharmaceuticals: A Detection Controlled Estimation Approach,” The Journal of Industrial Economics, 2018, 66 (4): 866–903. https://doi.org/10.1111/joie.12189; Tuba Tunҫel, “Should We Prevent Off-Label Drug Prescriptions? Empirical Evidence from France.” (Rochester, NY: Social Science Research Network, 2020), https://doi.org/10.2139/ssrn.3694632; David Paul Molitor, “Physician Behavior and Technology Diffusion in Health Care,” thesis, Massachusetts Institute of Technology, 2012, https://dspace.mit.edu/handle/1721.1/77795; Rebecca Jay McKibbin, “The Effect of RCTs on Demand for Off-Label Cancer Drugs,” (Rochester, NY: Social Science Research Network, 2020), https://doi.org/10.2139/ssrn.3574623.
[2]. David C. Radley, Stan N. Finkelstein, and Randall S. Stafford, “Off-Label Prescribing Among Office-Based Physicians.” Archives of Internal Medicine, 2006, 166 (9): 1021–26, https://doi.org/10.1001/archinte.166.9.1021; Ishaq Lat, et al., “Off-Label Medication Use in Adult Critical Care Patients,” Journal of Critical Care, 2011, 26 (1): 89–94, https://doi.org/10.1016/j.jcrc.2010.06.012.
[3]. Bradley T. Shapiro, “Informational Shocks, Off-Label Prescribing, and the Effects of Physician Detailing,” Management Science, 2018, 64 (12): 5925–45, https://doi.org/10.1287/mnsc.2017.2899.
[4]. The New York Times, “Opinion | Medicare and ‘Off-Label’ Cancer Drugs,” Editorial, February 10, 2009, https://www.nytimes.com/2009/02/10/opinion/10tue2.html.
[5]. Ian Larkin, et al., “Restrictions On Pharmaceutical Detailing Reduced Off-Label Prescribing Of Antidepressants And Antipsychotics In Children,” Health Affairs, 2014, 33 (6): 1014–23. https://doi.org/10.1377/hlthaff.2013.0939.
[6]. Shapiro, “Informational Shocks, Off-Label Prescribing, and the Effects of Physician Detailing.”
[7]. Blankart and Lichtenberg, “The Effects of Off-Label Drug Use on Disability and Medical Expenditure.”
[8]. M.-C. Husson, “Thériaque®: base de données indépendante sur le médicament, outil de bon usage pour les professionnels de santé,” Annales Pharmaceutiques Françaises, 2008, 66 (5): 268–77. https://doi.org/10.1016/j.pharma.2008.07.009.
[9]. Gautier Duflos and Frank R. Lichtenberg, “Does Competition Stimulate Drug Utilization? The Impact of Changes in Market Structure on US Drug Prices, Marketing and Utilization,” International Review of Law and Economics, 2012, 32 (1): 95–109, https://doi.org/10.1016/j.irle.2011.08.003.
[10]. Frank Lichtenberg, “Are drug prices subject to creative destruction? Evidence from the U.S., 1997-2017,” Health Economics, 2021, 30(8):1910-1932, August, http://doi.org/10.1002/hec.4283; Frank Lichtenberg, “The effects of dynamic and static competition on prescription drug prices in Denmark, 1997-2017,” Journal of Evolutionary Economics, June 28, 2022, https://doi.org/10.1007/s00191-022-00777-4.
